Enhancing Depth of Focus with Negative Spherical Aberrations: From Theory to Clinical Impact
The introduction of optical aberrations has become a prevalent approach in refractive and cataract surgery to enhance the depth of focus, compensating for the loss of accommodation associated with presbyopia. Negative spherical aberration (NSA), in particular, is widely employed in procedures like presbyLASIK and Extended Depth of Focus (EDOF) intraocular lenses (IOLs), where controlled induction of spherical aberration plays a key role. This page seeks to provide a refresher on the mechanisms involved in using negative spherical aberration and to clarify the conditions essential for its successful application—conditions that are often overlooked or even (deliberately?) obscured.
Core Concepts
The notion of optical aberration is as intuitive as it is abstract. In geometric optics, where the focus is on image location, size, and potential distortion, light is often represented as rays converging at a focal point. A wavefront is a virtual construction: it corresponds to the envelope of points in space that share the same phase, with variations represented by wave trains (sinusoids). A ray is another virtual construct that represents the local direction of the wavefront’s movement.
Vergence is a quantity expressed in Diopters, which is equal to the inverse of a distance. It is the refractive index of the propagation medium divided by the distance from (negative vergence) or towards (positive vergence) the focus. Thus, the farther from the source, the lower the vergence (in absolute value). If the source is at a great distance or infinity, the vergence incident on an optical element (diopter, lens) is zero. Vergence is a familiar concept for clinicians; reading a book requires a vergence of approximately 3 D (for a book positioned about 35 cm from the eye).
Rays represent the local propagation of the wavefront, which itself represents the envelope of points in the same phase state. In wave optics, the concepts of optical path and corresponding phase shift prevail. The distance between a wavefront and its focal point allows for the calculation of vergence, which involves its reciprocal and the refractive index of the medium considered.
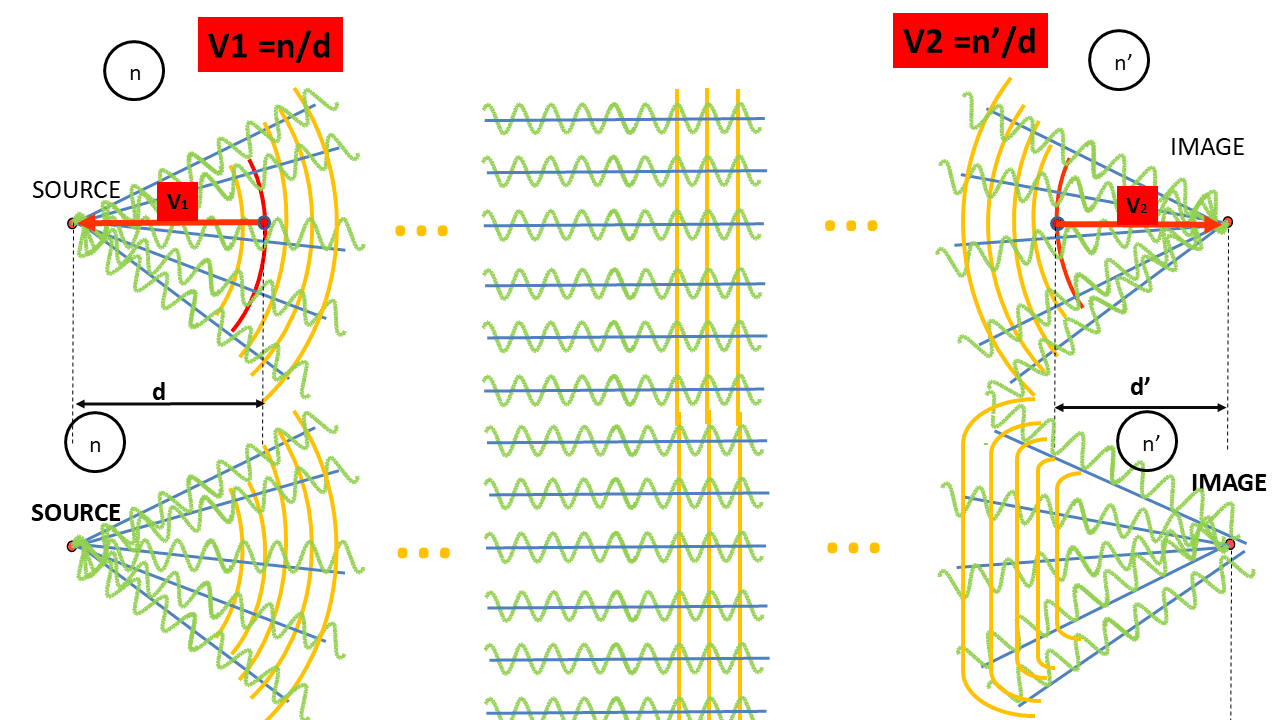
Consider a point source emitting light in all directions. We represent only part of the emitted light here in the form of wave trains, rays, and wavefronts, though our considerations will involve vergence. An optical system designed to converge light to a focal point can form an image of the point source from a portion of the captured wave/ray trains. Vergence is a paraxial concept, at least when using the vergence formula, though it can be extended to the wavefront envelope for didactic purposes. When the system is free of optical aberrations (top), vergence is the same for all points on a wavefront. In the presence of aberrations (bottom), the wavefront distortion causes vergence to vary at different points, as the envelope is no longer spherical (parabolic in the first approximation), and the physical distance of envelope points to the paraxial focus varies – These diagrams are not to scale.
Aberrations and their classifications aim to model and rationalize situations where there is an optical path difference between light from a source and the image plane, relative to an ideal optical system. The optical path concept naturally leads to phase difference and wavefront error surfaces.
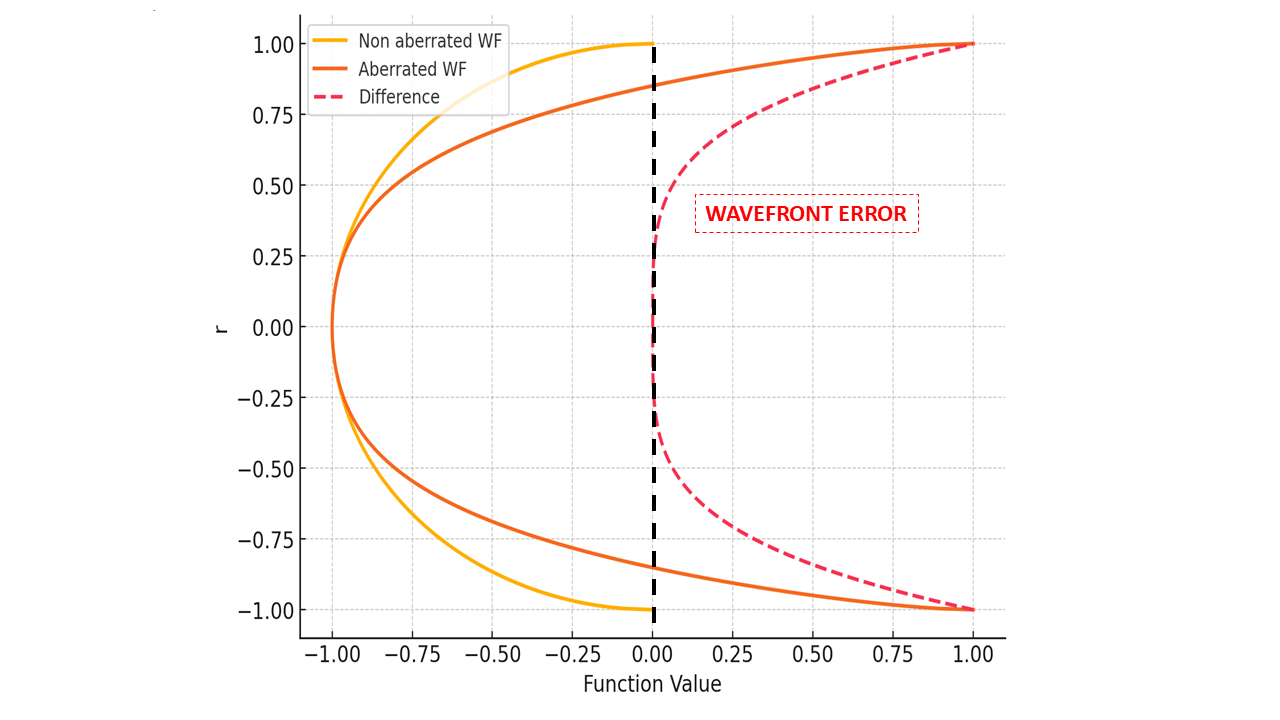
The study of the wavefront concerns the differences between the measured wavefront (with aberrations) and the ideal wavefront (reference). In this example, the difference is a pure fourth-degree spherical aberration. (the normalized pupil radius is plotted on the Y-axis)
As we will see, these optical path differences (in wavelength) or phase changes can also be translated into local power (vergence) variations, providing insight into the refractive impact of spherical aberrations.
For clarification, negative spherical aberration (NSA) in this context is measured in a setup where light rays emanate from a distant source (i.e., for “distance vision”).
Ray Tracing Representations of Negative Spherical Aberration
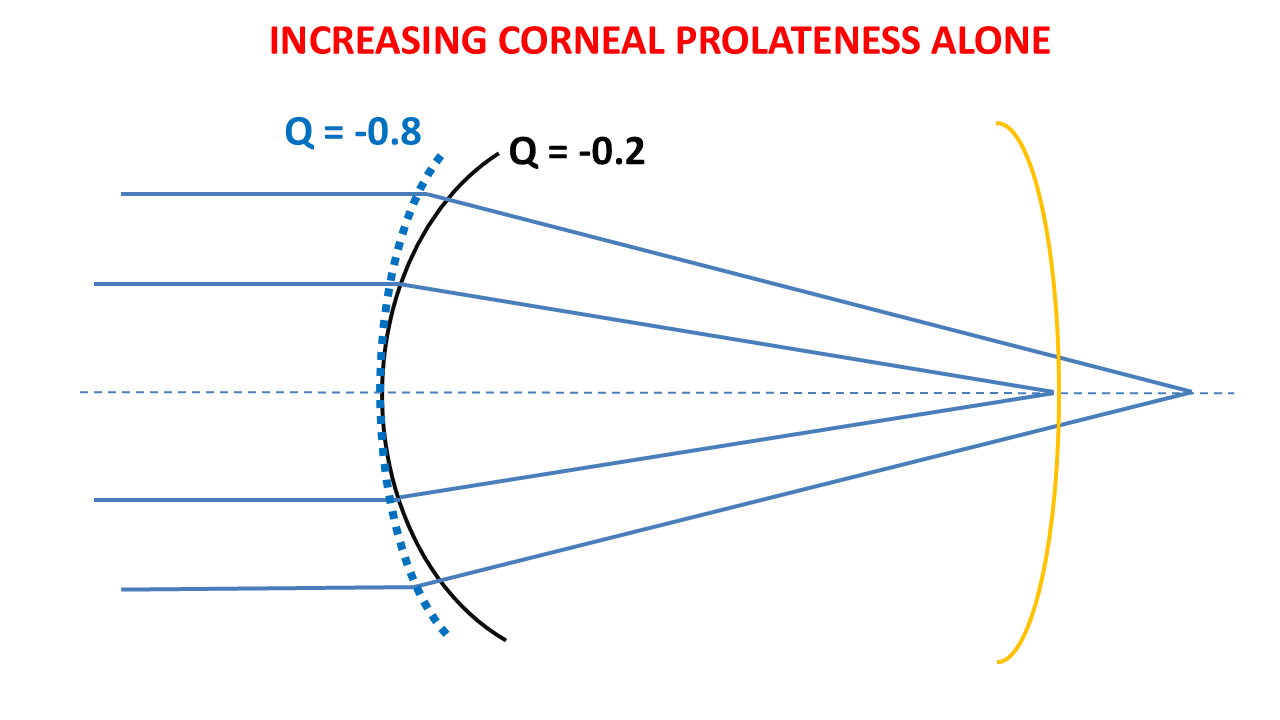
A simple way to represent NSA is through ray tracing in a biconvex symmetrical aspheric lens having two highly prolate surfaces.
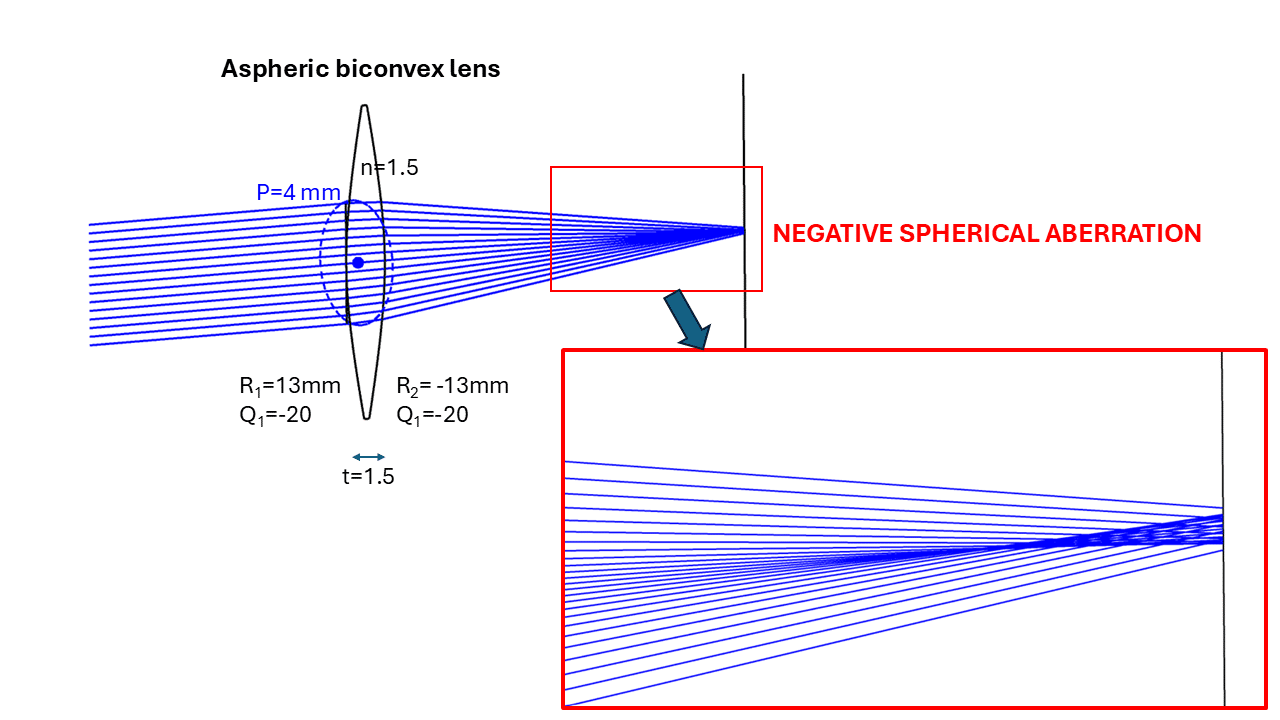
Biconvex lens with hyperprolate surfaces, generating negative spherical aberration. The enlarged detail reveals an area of light concentration (caustic). The image plane has been shifted away from the « best foci zone » to visualize the caustic better.
With NSA, paraxial rays—those close to the optical axis—converge first, forming a proximal focal point zone. In contrast, rays farther from the axis are refracted at a greater distance, creating a pattern called « a caustic. » This pattern indicates an area where light is concentrated enough to form an interpretable image of sufficient quality in a plane that would intersect the caustic.
NSA fundamentally represents a gradual focal length increase for peripheral rays, illustrating a consistent defocusing progression as rays become more peripheral.
Through focus spot diagrams are valuable tools for visualizing how an optical system focuses light from different field angles or object distances. By plotting the distribution of light spots on a focal plane, these diagrams reveal the presence and impact of optical aberrations, such as spherical aberration:
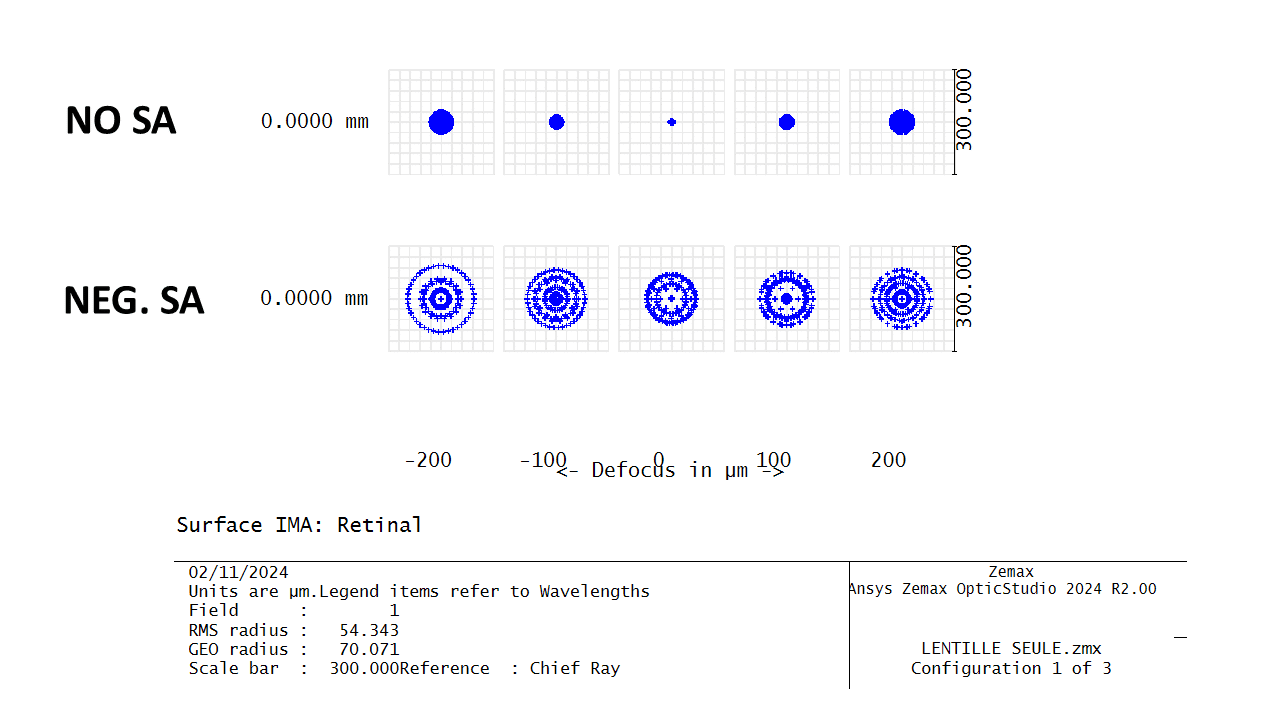
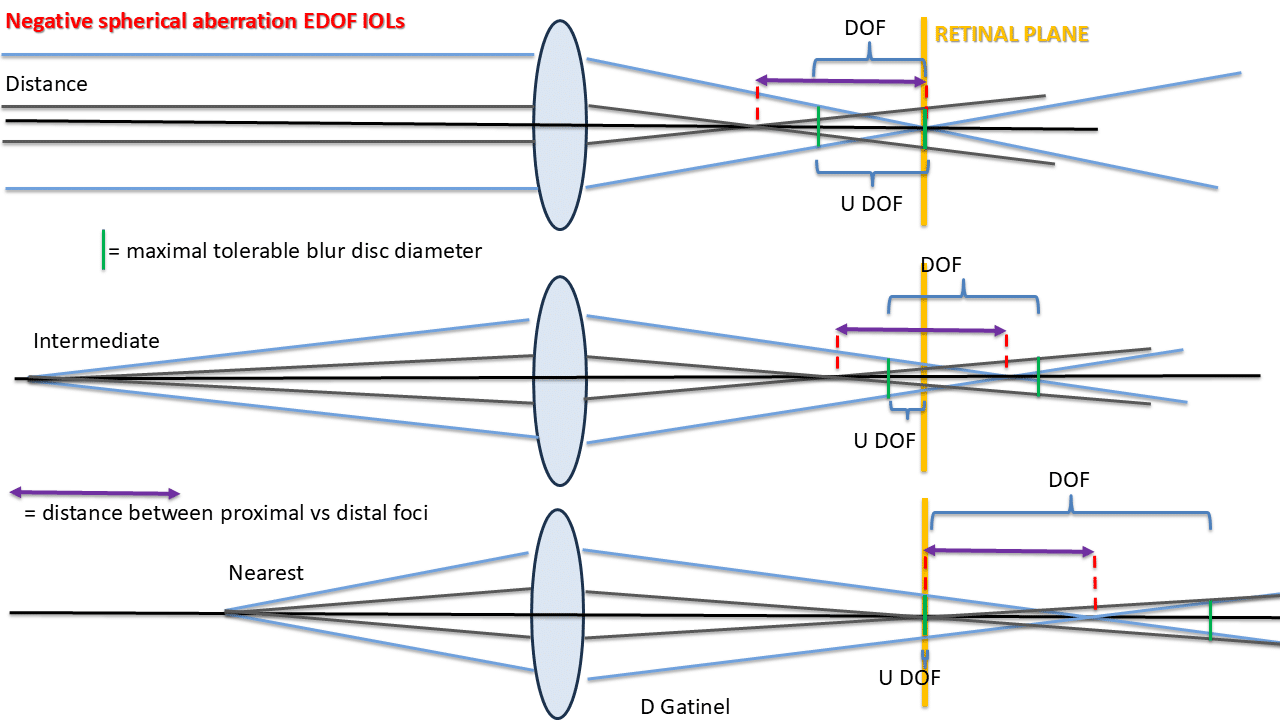
Comparison between a lens corrected for spherical aberration and a lens with negative spherical aberration. Optical performance is reduced in the latter case but remains relatively stable across different defocus values. The effective depth of field depends on the maximum tolerable blur spot diameter and the position of the focal points within the interval where blur remains below this diameter. Ideally, these points should be located in front of the retinal plane for rays originating from a distant source—or behind it for rays from the nearest target that still appears sufficiently clear.
A “functional” representation of NSA would be beneficial in clinical applications aimed at providing sufficient vision across various distances for presbyopic eyes. It is ideal for variable distance-situated sources to yield a sufficiently concentrated image plane (retinal) focus.
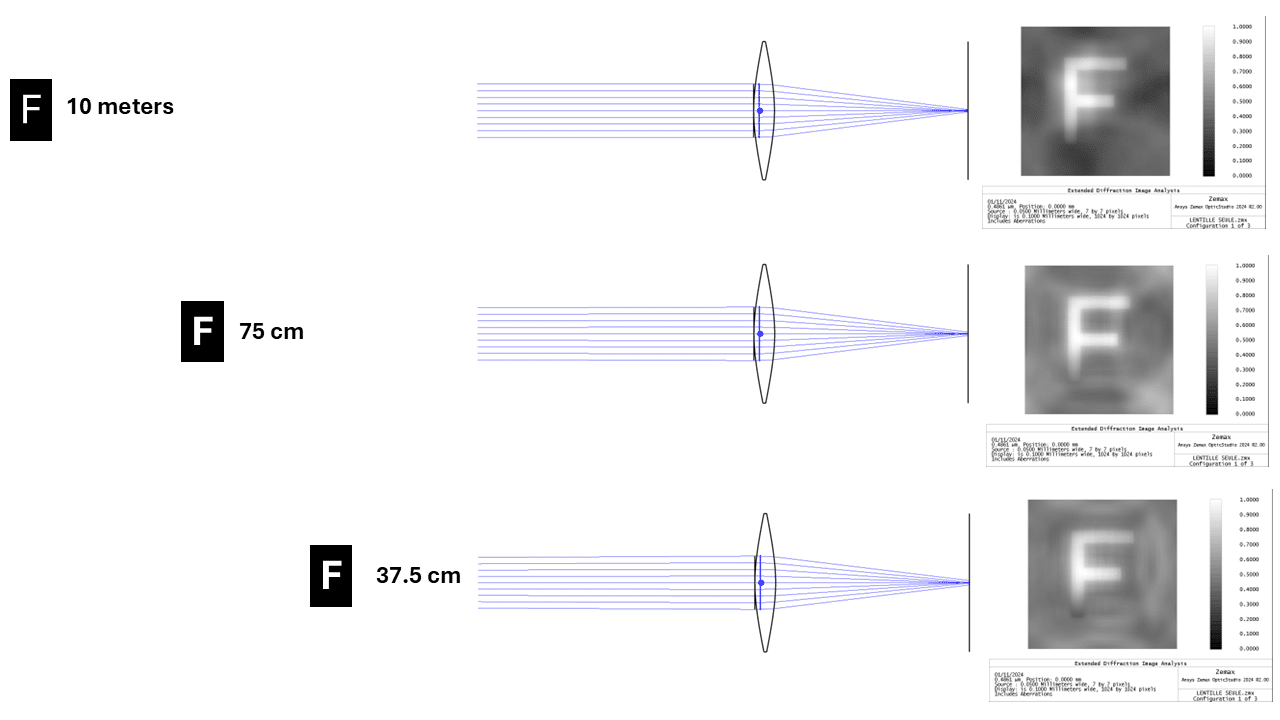
Simulations for different target distances with the previous Negative spherical aberrated lens. The letter is identifiable despite the overall reduction in contrast that is already noticeable for the distant target (10 meters). Interestingly, the rays that help preserve detail for the image of the target from a distance are refracted at a distance from the optical axis. The closer the targets are, the closer the rays are focused in the image plane to the optical axis.
Importantly, NSA alone does not extend the depth of focus in an emmetropic eye (in which paraxial rays are focused in the retinal plane) and can degrade optical quality without improving near vision at all! Indeed, if paraxial rays from a distant source produce emmetropia, non-paraxial rays will be defocused onto a plane located behind the retina. This will inevitably be the case for all rays from nearby sources, as they will have a divergent incidence!
Conversely, if rays refracted paracentrally by a nearby target are conjugate with the retina, this refraction can, by definition of myopia (punctum remotum located at a finite distance), be considered myopic. In this configuration, the superimposition of these paracentral rays, defocused in front of the retina, with fewer paracentral rays gradually focused on the retinal plane should allow for sufficiently clear distance vision (controlling the induced blur).
Seidel’s Classification and Spherical Aberration
Seidel’s classification is simple but effective, defining spherical aberration as:
W(r) = a40 ⋅ r4
a40 is a weighting coefficient. This function describes the wavefront deviation due to spherical aberration. For negative SA : a40 < 0
The r4 term designates spherical aberration as a fourth-order aberration. This wavefront error map reflects the gradual defocus of rays as they are refracted further from the optical axis.
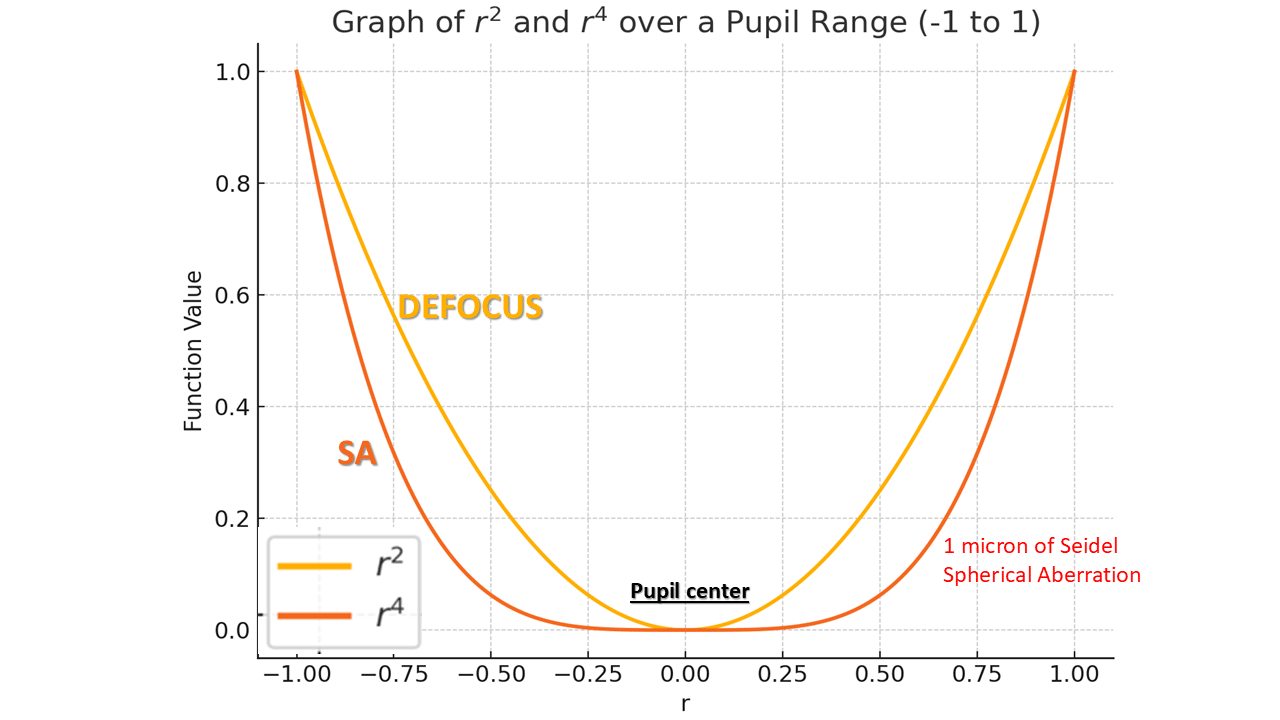
Spherical aberration is a wavefront error of the fourth order (radial degree 4). This wavefront error primarily affects the edge of the pupil, unlike defocus aberration (degree 2), which impacts the entire pupil area. For a small pupil diameter, the expected impact of Seidel-type spherical aberration on subjective refraction is negligible. Towards the pupil edges, the effect of spherical aberration adds to that of defocus if they share the same sign. If defocus is positive (indicating myopia, by convention) and the spherical aberration is also positive, myopia increases at the pupil periphery. In this case, vergence is no longer uniform across the pupil. Conversely, if defocus is negative (indicating hyperopia) and spherical aberration is negative, the hyperopic defocus intensifies towards the edges.
The wavefront error due to NSA increases slowly initially, accelerating at the pupil’s edge, a hallmark of high-order aberrations in ophthalmology. Although Seidel-like NSA’s effect on refractive error is limited—particularly since central rays largely determine clinical refraction—the peripheral defocusing typical of an emmetropic eye can reduce retinal image quality (contrast) by shifting peripheral ray focus behind the retina.
Zernike Spherical Aberration
The representation of spherical aberration in the Zernike classification is more complex, if not problematic. This is due to reasons that we won’t elaborate on here but which relate to the need for these functions to possess certain mathematical properties that, while desirable in instrumental optics, are less suitable in clinical ophthalmology. Put bluntly, the representation of negative spherical aberration in the Zernike classification undermines the very principle of effectively segregating aberrations that can be corrected with glasses (second-degree) from those that cannot (fourth-degree).
The Zernike polynomial Z40 with normalization coefficient is:
Z40(r) = √5 * (6r4 – 6r2 + 1)
Where:
- r is the normalized radial coordinate (0 ≤ r ≤ 1).
- The coefficient √5 is the normalization factor.
One need only compare the wavefront error equation with that of the Seidel classification to observe an oddity. Here, NSA is expressed with a second-order term (defocus) opposite in sign to the primary fourth-order term. There is also a constant term, which has no impact on the optical plane and exists solely due to analytical constraints that are largely irrelevant in a clinical context.
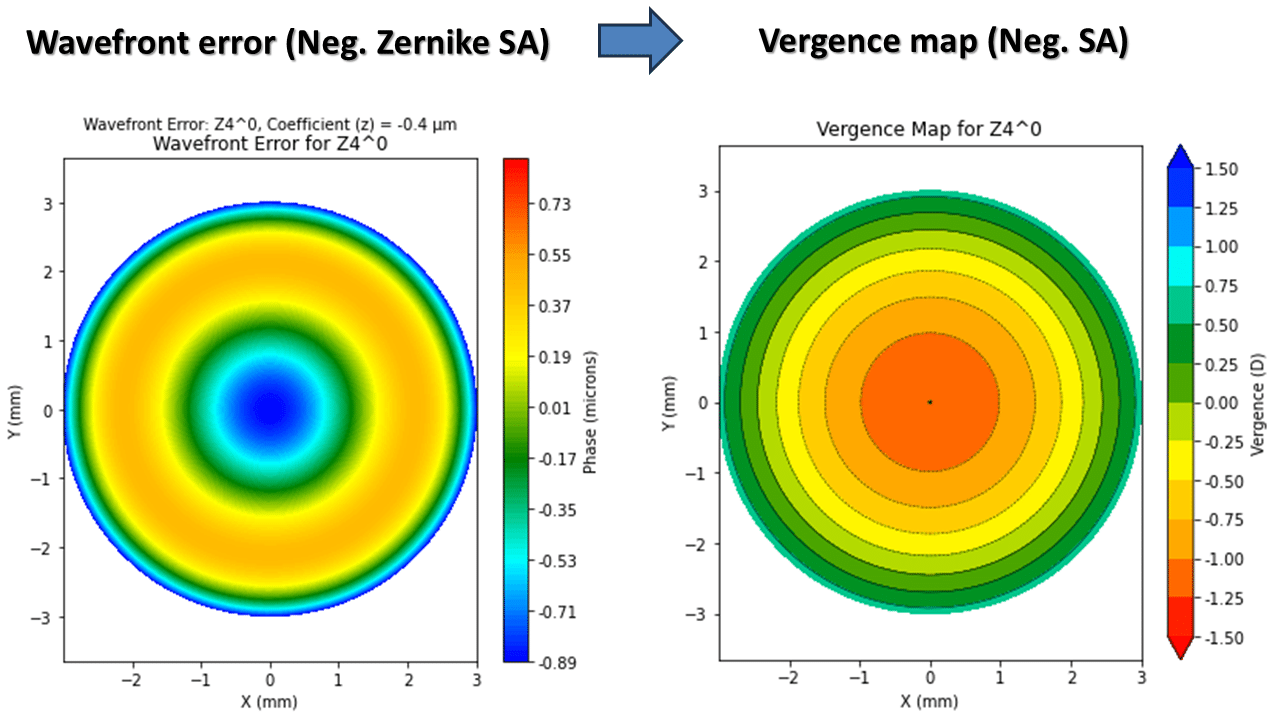
This helps explain why the Zernike fourth-degree spherical aberration takes on this “sombrero” shape: the central bulge corresponds to the influence of the second-degree term, dominating at the center over the fourth-degree term, which only prevails from outside the outer third of the pupil diameter.
The presence of this defocus term is far from incidental—quite the opposite. A simple analytical study shows that for a coefficient z40 of 1 micron of Zernike spherical aberration, there are over 4 microns of associated defocus of the opposite sign! The impact of defocus within that Zernike mode is naturally proportional to the coefficient that scales it. In the context of presbyopia compensation, where this coefficient is deliberately increased to more negative values, it cannot be ignored. For 0.25 microns of negative spherical aberration with a 6 mm pupil, the amount of defocus present (about 1 micron) corresponds to at least +0.75D of positive defocus (myopia).
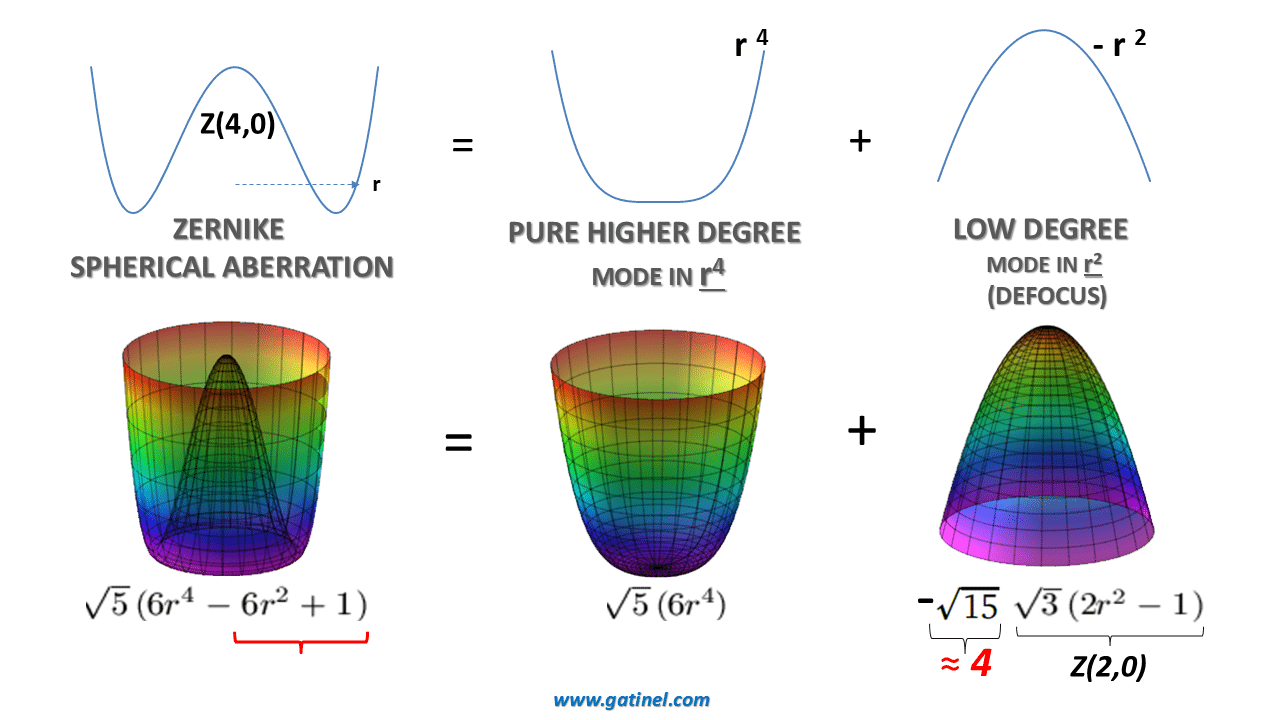
Here is represented the decomposition of the Zernike 4th order spherical aberration Z40 mode with a coefficient of 1 micron into a component in r4 and a component in r^2 …which is equivalent to roughly 4 microns of Zernike defocus Z20^!
In the Zernike convention, a negative defocus (Z20) coefficient corresponds to hyperopic refraction, and vice versa. Thus, positive spherical aberration includes a hyperopic refraction component, while negative spherical aberration includes a myopic refraction component. Subjective refraction primarily depends on the central region of the pupil, so any variation in wavefront error at this level significantly impacts the performance of the eye. Defocus leads to a marked reduction in the transmission of high spatial frequencies, which encode image detail. Achieving good uncorrected visual acuity requires a “flat” wavefront in the central pupillary region.
This blending of terms is a source of conceptual confusion and errors, which can be even more problematic as it sometimes allows certain stakeholders to exploit the resulting ambiguity to exaggerate the benefits of negative spherical aberration (NSA) and obscure some of the inherent constraints in effectively using NSA to compensate for presbyopia.
When studying the impact of Seidel-type spherical aberration on refraction, it is noted that for negative values, a slight hyperopic shift will be observed. This reflects the effect of reduced power toward the pupil periphery, even though the refraction in the paraxial zone remains unchanged. However, if Zernike negative spherical aberration is induced, the opposite effect will be seen due to the positive defocus (myopic shift) introduced by this aberration. This is a common source of confusion and can lead to partially incorrect interpretations, especially concerning Extended Depth of Focus (EDOF) implants, as highlighted in a recent letter to the editor.
To address this issue more clearly, we must return to a more clinical understanding of what high-order aberrations represent for a system’s optical properties.
Wavefront Error and Vergence Map
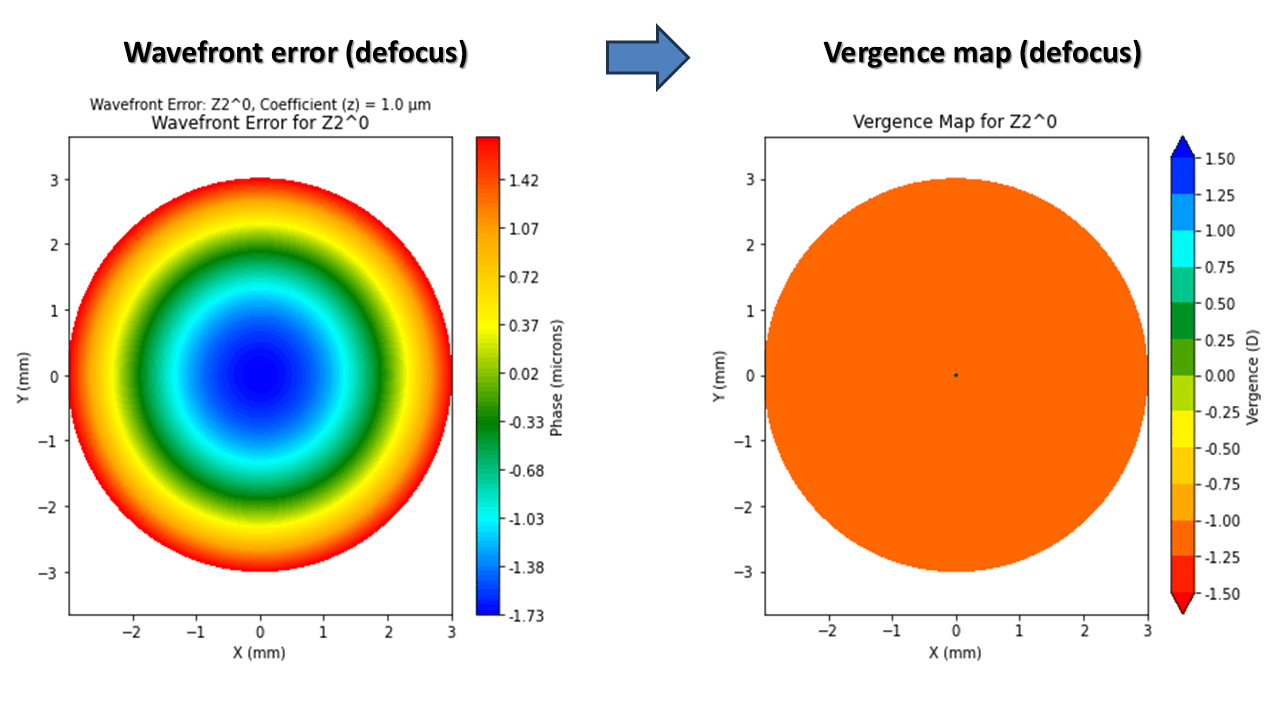
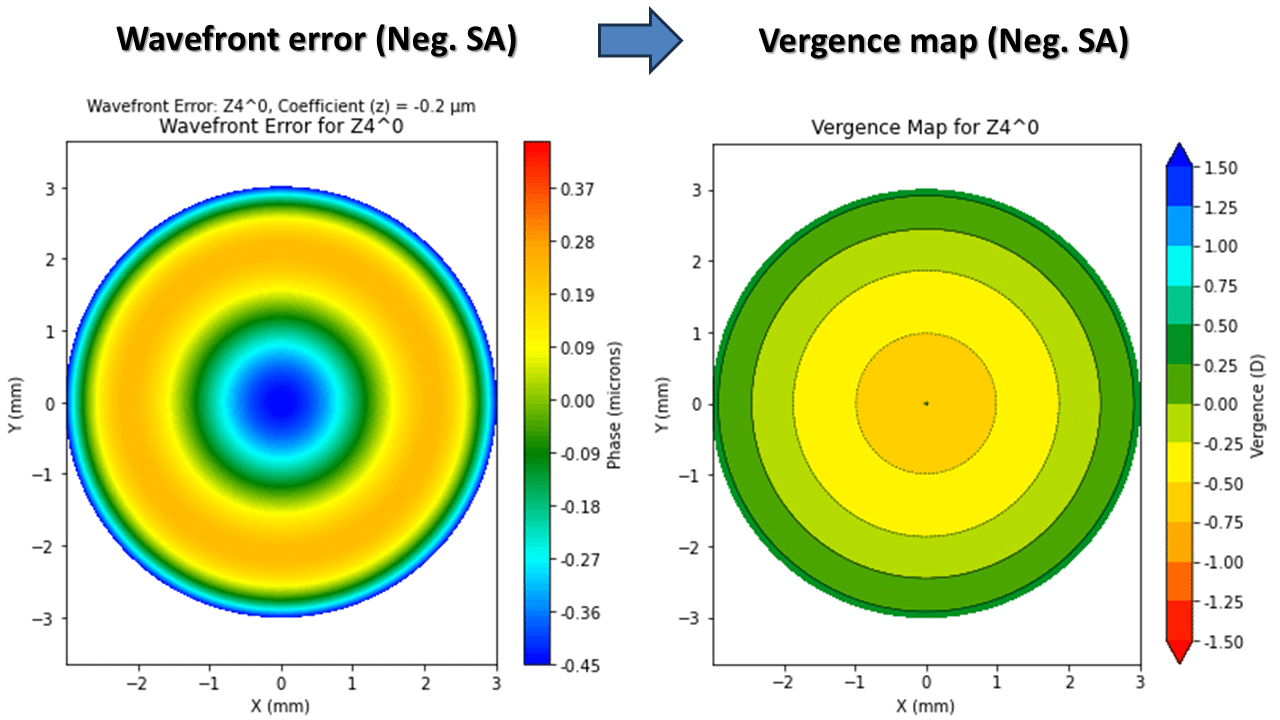
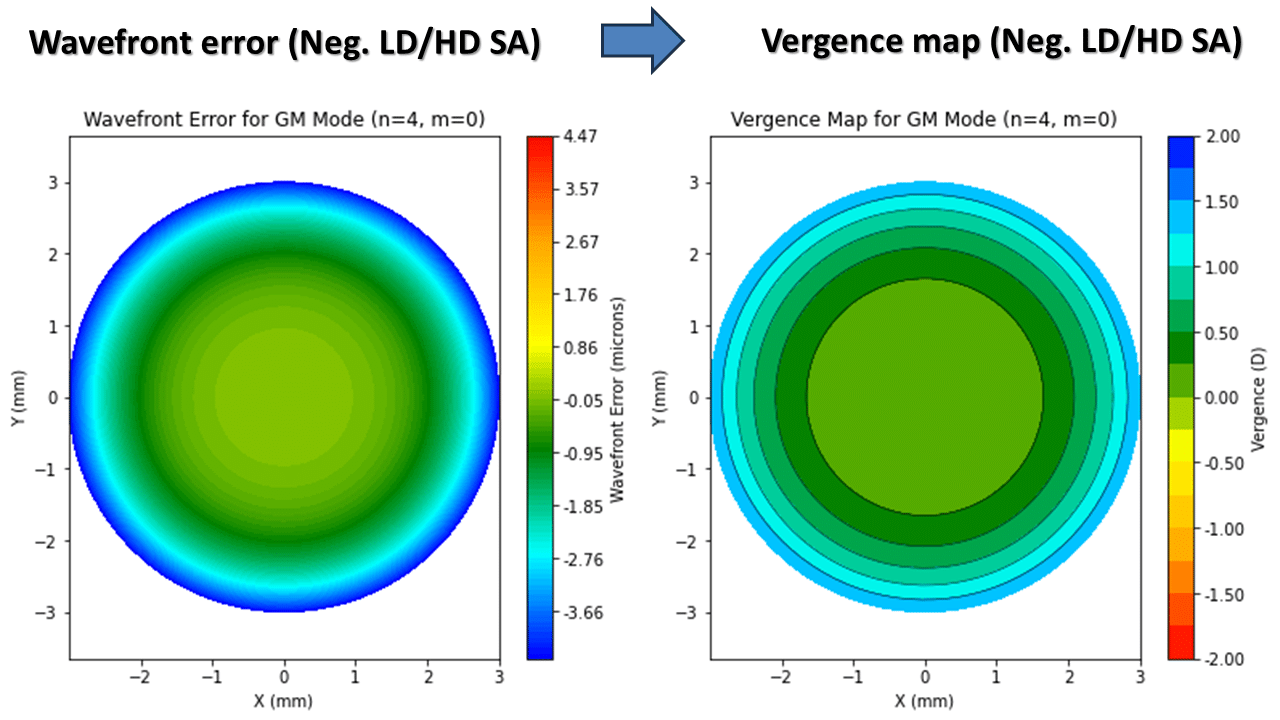
On the left is a wavefront error map corresponding to -2 microns of spherical aberration of the LD/HD type. On the right, the map of correpsonant vergence shows a gradient of about 2 D of hyperopia (central emmetropia, and hyperopia towards the edges of the pupil). This aberration, pure in higher-order terms, does not induce any significant variation in paracentral refraction.
Conclusion
In conclusion, a solid understanding of the theoretical foundations of optical aberrations—particularly negative spherical aberration (NSA)—is crucial for effectively applying these concepts in clinical settings. As the management of presbyopia increasingly incorporates controlled optical aberrations to extend depth of focus, comprehending the underlying mechanisms becomes essential. NSA, widely used in presbyLASIK and EDOF IOLs, offers significant potential for enhancing vision across varying distances, but only if applied with a precise awareness of its effects on vergence and image quality across the pupil.
It is essential to clearly understand the type of spherical aberration being referenced when a study or a promoter discusses its use for presbyopia compensation. Different types of spherical aberration, such as Seidel or Zernike, have distinct optical effects and implications. Misunderstanding the specific type can lead to incorrect assumptions about the expected clinical outcomes, making it crucial for practitioners to recognize which form of spherical aberration is being applied in each context.
This page aims to demystify the optical and refractive implications of Negative SA, illustrating how theoretical principles translate into clinical practice. By bridging these foundational concepts with practical application, ophthalmologists can better tailor their approach to presbyopic correction, balancing the trade-offs between distance clarity and extended near focus. Ultimately, such a nuanced understanding supports the development of optimized, patient-specific strategies that maximize visual outcomes in refractive and cataract surgery.
Related content and useful references
Numerous studies have explored the impact of spherical aberration on visual quality, spherical-cylindrical refraction, and depth of field. I encourage you to consult these resources if you’re curious and wish to delve deeper into this important field.
The following parameters have been taken into consideration in some studies:
- The influence of individual pupil dynamics in each eye
- The metrics employed (Strehl ratio, convolved images, MTF, etc.)
- The range of spatial frequencies considered
- The « Crawford effect » (attenuation of peripheral rays’ impact)
- Biometric characteristics (e.g., the influence of anterior chamber depth in pseudophakic eyes)
Can you recommend ‘hyper prolate contact lens?
Currently using aquacomfort multifocal hi center near, adjusting my script so peripheral power = my refracted power. As per a paper it has steep power profile all the way to edge
What’s difference between center near flat central with steep periphery vs steep central and flat periphery?
√5 * (6r4 – 6r2 + 1) is not equal to √5 * (6r4) – √15*√3(2r2 – 1)
What are the complications of BVI Isopure IOL?